Health professionals worry about patients who receive false diagnoses and who are pursuing unproven and disproven therapies.
Real infections have been hijacked by a pseudoscientific belief system, so it’s difficult to determine what is true and not true. Chronic Lyme quackery should not be confused with real Lyme disease or symptoms that can occur after treatment.
According to the American Academy of Pediatrics:
The long-term prognosis for individuals who are treated appropriately with antimicrobials for Lyme disease, regardless of the stage of the illness, is excellent. The most common reason for a lack of response to appropriate antimicrobial therapy is misdiagnosis (ie, the patient actually does not have Lyme disease).
Nonspecific symptoms, such as fatigue, arthralgia, or myalgia, may persist for several weeks even in patients with early Lyme disease who are treated successfully. Their presence should not be regarded as an indication for additional treatment with antimicrobials. These nonspecific symptoms will usually resolve without additional antimicrobial therapy.
There is substantial evidence that there is no such entity as chronic Lyme disease. Indeed, there is not even a case definition for chronic Lyme disease. There are many websites that contain misinformation about Lyme disease that only enhance the already inflated and inaccurate fears about the consequences of Lyme disease of many parents and patients.
Many patients labeled as having chronic Lyme disease actually have medically unexplained symptoms. Such patients are best treated symptomatically rather than with prolonged courses of antimicrobial therapy, which have been associated with serious adverse effects and little or no benefit. It is important to acknowledge that the patient has symptoms even if they are not due to Lyme disease.
Table of contents
Deceptive marketing terms
The most popular marketing terms used by modern peddlers of health scams are integrative, functional, and naturopathic. They often falsely claim to get to the “root cause” of problems, whereby patients are tricked into purchasing fake tests, fake diagnoses, and fake treatments.
With respect to chronic Lyme quackery, the perpetrators will usually be marketed as “Lyme literate” or as a “Lyme specialist”. Lyme—and easily-debunked conspiracy theories surrounding it—became the hook for an alternate universe that sucks people in and can ruin their lives.
Fake co-infections
In the 1990s, “Lyme literate” leaders expanded their grift to include so-called co-infections. Fraudulent co-infection diagnoses are inspired by genuine but uncommon instances where a single tick could transmit multiple infections simultaneously.
But authentic co-infections are different from authentic Lyme disease. The “Lyme literate” fraudsters will diagnose co-infections that have never been credibly documented like Lyme-bartonella or babesia-bartonella. CDC reported on fraudulent Lyme-Babesia co-infection diagnoses facilitated by antibody tests even though mainstream labs can directly detect real Babesia parasites with microscopy and PCR.
For lab testing for Lyme disease, experts recommend antibody tests, in the appropriate context. While direct detection has been used in research studies, it is not considered sensitive enough for routine diagnosis in the clinic. Pseudoscience advocates will often claim that a sensitive direct test will solve the “problem” of mainstream testing contradicting their diagnoses. But as can be seen with the bogus Babesia diagnoses, the true problem is false beliefs, not whether a perfect direct test is available.
Attempts to rebrand
Advocates for the false “Chronic Lyme” and co-infections diagnoses know that mainstream science doesn’t recognize them, so they will often use other terminology like “persistent Lyme”, “late stage Lyme,” “Lyme borreliosis complex,” “Lyme+”, “Long Lyme,” or just Lyme.
One of the most notorious “Lyme literate” charlatans, Richard Horowitz, MD, invented a marketing term he called MSIDS (Multiple Systemic Infectious Disease Syndrome).
In the wake of the COVID-19 pandemic, advocates for chronic Lyme pseudoscience attempted to legitimize themselves by co-opting concerns about COVID sequelae, otherwise known as Long COVID. Conspiracy theorists and those funded by them promoted the term “infection-associated chronic illnesses.”

Many stories of false chronic Lyme diagnosis exhibit red flags, which are listed below. However, just because there is a noticeable red flag, it does does not necessarily mean a diagnosis or treatment is inappropriate.
Quotes from healthcare organizations:
Antibiotics are the only known effective treatment for Lyme disease, but a quick search on the internet will introduce you to other untested remedies that claim to cure Lyme disease or chronic Lyme disease. These products—available online or from some health care providers—may be dangerous, deadly, or simply a waste of money.
— CDC (Alternative treatments)
We sympathize with patients who suffer from the wide array of symptoms that have been attributed by some to be due to so-called “chronic” Lyme disease, but we are concerned that most of these patients have been improperly diagnosed and may be receiving a treatment, i.e., long-term antibiotic therapy, that will do them more harm than good.
— Infectious Diseases Society of America (IDSA Letter to Congress, 2009)
Major red flag: “Chronic Lyme” where real Lyme is rare or non-existent
Chronic Lyme is a social phenomenon spread by word of mouth and the Internet. Thus, chronic Lyme is not restricted to areas where ticks transmit the curable Lyme infection.
With real Lyme disease, 95% of reported US cases are in 14 states, mostly in the Northeast, mid-Atlantic, and Upper Midwest.
Healio’s excellent article on the misnomer of chronic Lyme disease features this graphic illustrating the stark difference in geography between confirmed Lyme cases and chronic Lyme support groups:
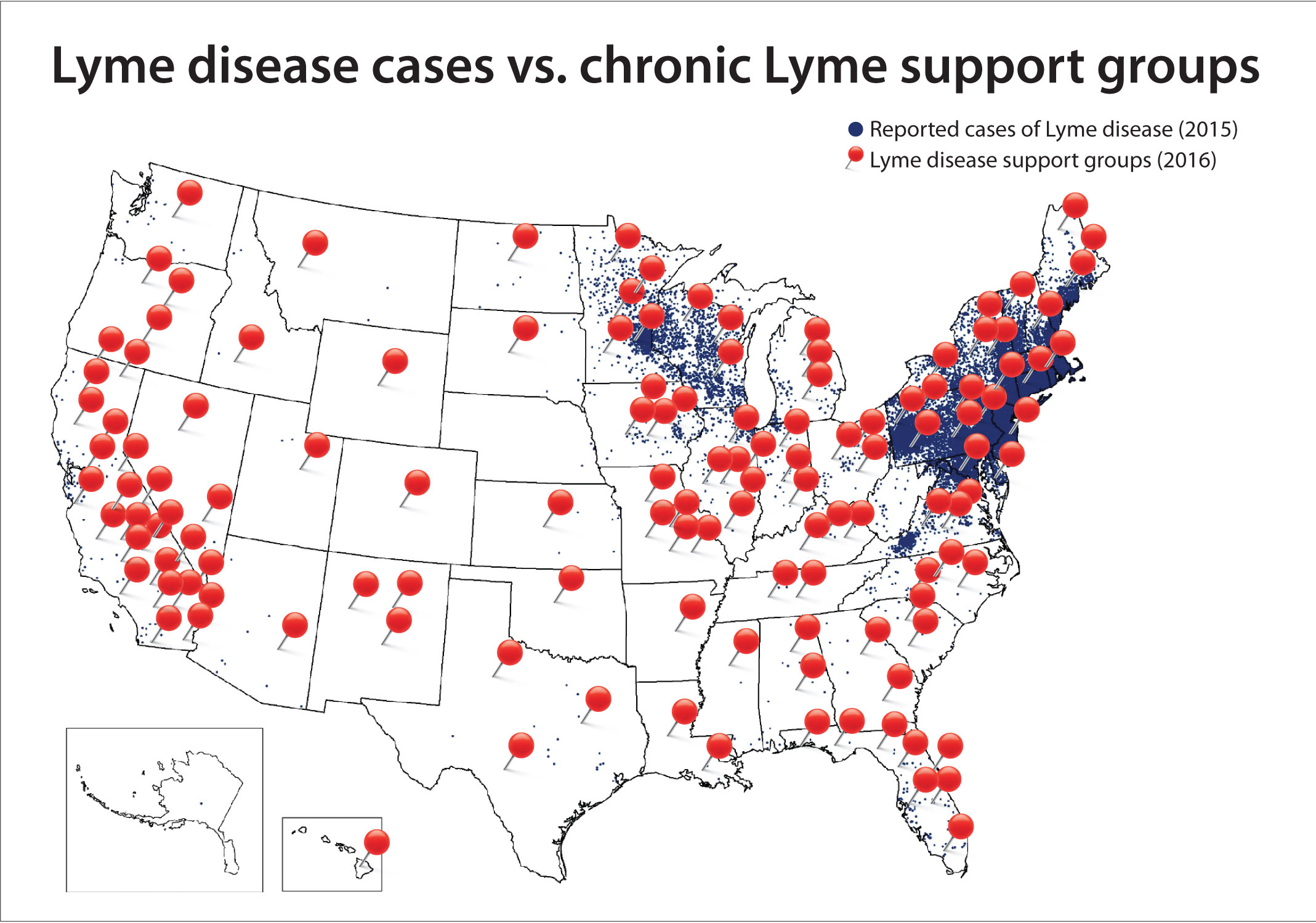
The United States has exported its conspiracy theories about Lyme disease to many countries, including Canada, UK, France, Germany, Poland, Spain, and Turkey. Thousands of people have received false diagnoses in Australia, where there is no endemic Lyme disease.
Major red flag: Unscientific medical practitioners
- Including those who market themselves using the following terminology: Lyme literate (especially those affiliated with ILADS and ISEAI), integrative, functional, alternative, complementary, Traditional Chinese Medicine, holistic, natural, Biological, Ayurvedic, chiropractic, naprapathic, homeopathic, anti-aging, regenerative (private practice), environmental (private practice), and naturopathic.
- Including members of organizations listed as “questionable” by Quackwatch, such as the American Academy of Environmental Medicine.
- A surprising number have had a personal experience where themselves or a loved one received a fictional diagnosis.
- They frequently profit from sales of unproven or disproven treatments like herbs and supplements, a practice that naturopathic whistleblower Britt Hermes deemed unethical.
- Treatments may be marketed for unrelated diseases, for example both Lyme disease and cancer.
A warning from Dr. James Hamblin, MD, preventive medicine physician and staff writer at The Atlantic:
There aren’t many absolutes in medicine but one is never trust a doctor who has their own line of dietary supplements.
Diagnosis Red Flags
- Doctor shopping (including traveling a long distance to a “Lyme specialist”)
- Implausible coinfections (MSIDS, Bartonella, chronic babesia, chronic ehrlichia, tick-borne mycoplasma, “toxic mold” (aka biotoxin illness or CIRS-Chronic Inflammatory Response Syndrome), MARCoNS, unsubstantiated Epstein-Barr/mononucleosis, heavy metals, Protomyxzoa rheumatica (aka FL-1953), WiFi/EMF sensitivity, Morgellons, and others)
- Claiming that harmless stretch marks or neuropsychiatric symptoms are a bartonella infection
- Claiming that nonspecific symptoms like “air hunger” and shady antibody tests (rather than PCR or visual observation of a blood smear performed in a mainstream lab) are sufficient to diagnose Babesiosis
- Unsubstantiated claims of Mast Cell Activation Syndrome (MCAS, see consensus, and paper)
- Coinfections that aren’t transmitted together, that are rare, and would be readily treated if real
- Claiming to have contracted Lyme disease in a location where Lyme disease is rare or non-existent
- A long list of non-specific symptoms attributed to Lyme disease, including useless questionnaires distributed by chronic Lyme advocates, such as Joseph Burrascano and Richard Horowitz (HMQ: Horowitz MSIDS Questionnaire)
- Attempting to blame an established disease or disorder on Lyme disease, despite no link
- “Lyme literate” charlatans have defrauded and abused people with Multiple sclerosis, ALS, autism, Parkinson’s, Alzheimer’s, auto-immune diseases, and many other conditions.
- Medically unexplained physical symptoms, such as chronic fatigue syndrome and fibromyalgia, are frequently falsely blamed on Lyme disease.
- Claiming that mental health symptoms are evidence of Lyme disease (Experts agree: “No studies suggest a convincing causal association between Lyme disease and any specific psychiatric conditions.”)
- Ignoring a plausible diagnosis from mainstream medical providers
- A belief that one or more infections occurred years earlier, or even in utero
- The longer someone has had symptoms, the less likely Lyme is to be the culprit. (source)
- Unsubstantiated claims of being immunocompromised, or that Lyme has caused immunosuppression or “B-cell AIDS”
- Unvalidated tests (e.g. CD57, urine tests, Lymphocyte Transformation Tests (LTT), ELISpot/interferon gamma tests/LymeSpot and other assays based on T-cell activity, Live blood cell analysis, Phelix Phage test, circulating immune complexes (in Poland, KKI or Krążące kompleksy immunologiczne), proprietary interpretations of standard tests, electrodermal devices that use skin conductance or impedance like Meridian Stress Assessment (MSA) and ZYTO, Visual Contrast Sensitivity testing (VCS))
- Shopping for positive lab results from far-away labs (e.g. from Germany or the United States) that use unvalidated tests
- Any other testing that is not FDA-cleared and CDC-recommended (with the exception of mainstream European testing appropriately used for suspected European Lyme)
- Definitive clinical diagnosis of late Lyme disease without supporting mainstream testing
- Tests from any of the following labs or lab-associated entities: IgeneX, DNA Connexions, Galaxy Diagnostics, Medical Diagnostic Laboratories (MDL), Milford Molecular Diagnostics Laboratory, Advanced Lab*, Fry Laboratories, Ceres Nanosciences (Nanotrap), Global Lyme Diagnostics*, Pharmasan Labs (iSpot Lyme)*, Coppe Laboratories (myLymeTest*), ArminLabs, i-Labs (successor to Infectolab Americas, Infectolab, BCA-Clinic, and BCA-lab), Australian Biologics, Melisa Labs, Moleculera Labs (Cunningham Panel), R.E.D. Labs, Immunosciences Lab, Aperiomics*, Te?ted Oy (Tezted Limited, TICKPLEX), Lyme Diagnostics Ltd. (DualDur cell technology), Phelix, ProGene (DX Genie), Ionica Sciences (IonLyme)*, T Lab Inc, Veramarx, Vibrant America/Vibrant Wellness, Research Genetic Cancer Centre (RGCC)/Biocentaur (PaLDiSPOT, PrimeSpot), Deutsches Chroniker Labor (B16+ test), Nordic Laboratories, IncellDX, Dedimed GmbH Europarc Labor (AK-18Save), IgeneX-associated Acudart Health, Alianza Biohealth, Rupa Health (part of Fullscript), Universal Diagnostic Laboratory, Mosaic Diagnostics (formerly Great Plains Laboratory), any lab on Quackwatch’s list of “Laboratories Doing Nonstandard Laboratory Tests“. (Starred labs or tests are defunct)
- Multiple Lyme and/or other tick-borne disease tests performed more than 6 weeks after symptoms appeared
- Ignoring or misinterpreting non-positive antibody tests. Examples include:
- Using the IgM Western blot test more than 30 days after the appearance of symptoms
- Ignoring or failing to perform the first tier ELISA test
- Misinterpreting fewer than 5 bands on the IgG Western blot as positive (especially band 41, which is commonly positive in healthy people)
- Interpreting faint (but negative) Western blot bands as positive
- Using non-standard Western blot bands such as bands 31 and 34
- Ignoring a negative test based on false rumors about the test performance, given that “Immunoglobulin G (IgG) seronegativity in an untreated patient with months to years of symptoms essentially rules out the diagnosis of Lyme disease, barring laboratory error or a rare humoral immunodeficiency state.”, according to the 2020 consensus guidelines.
- Misinterpreting persistent antibodies as persistent infection after a cured infection or asymptomatic infection that the immune system cleared on its own
- ⭐ LymeScience: Further explanation of misinterpretation of mainstream tests
- A diagnosis that involves a psychic, reiki/energy healer, shaman, or practitioner of muscle testing (aka ART-Autonomic Response Testing or applied kinesiology)
- Encouraging tick testing (which experts recommend against) and making a diagnosis based on tick testing rather than compatible symptoms and validated diagnostic criteria
- Claiming that a patient must perform a ritual (e.g. exercise) to provoke and bring out the bacteria prior to testing
- Inappropriate use of medical imaging (e.g. SPECT scans or dark field microscopy aka Live Blood Analysis)
- Claiming that Lyme is transmitted sexually, congenitally, via breast milk, or any other method other than via a black legged (Ixodes) tick
- Falsely claiming that CDC-recommended testing is not for diagnosis and only for surveillance (rather than for both, as is the reality)
- Mixing anti-vaccine and Lyme conspiracy theories to support a diagnosis
- Falsely claiming that CDC-recommended testing was changed because of the Lyme disease vaccine (It was not changed at all)
- Falsely claiming that vaccines cause or trigger Lyme disease
- Claiming to be “CDC positive”
Treatment Red Flags
- Bizarre drug regimens (including non-standard antibiotics)
- Long-term antibiotics
- An overwhelming scientific consensus supports 10-28 days of generic antibiotics for Lyme disease. On rare occasions, a second course is used “with objective signs of relapse” (e.g. arthritis, meningitis, or neuropathy), as discussed in the 2020 consensus guidelines.
- Further, the 2020 consensus guidelines state: “For patients who have persistent or recurring nonspecific symptoms such as fatigue, pain, or cognitive impairment following recommended treatment for Lyme disease, but who lack objective evidence of reinfection or treatment failure, we recommend against additional antibiotic therapy (strong recommendation, moderate-quality evidence).“
- “Pulsed dosing in which antibiotics are given on some days but not on other days” († quoted from box 2 of a 2016 review)
- “Multiple repeated courses of antibiotics for the same episode of Lyme borreliosis”†
- “Combinations of antibiotics”†
- “First-generation cephalosporins, such as cephalexin, benzathine penicillin G, fluoroquinolones, carbapenems, vancomycin, metronidazole [aka Flagyl], tinidazole [aka Tindamax], trimethoprim-sulfamethoxazole [aka Bactrim, Septra], amantadine, ketolides, isoniazid, rifampin or fluconazole”†
- Minocycline
- Cefdinir
- Dapsone
- Disulfiram (aka Antabuse)
- Methylene blue
- Cholestyramine
- Loratadine (aka Claritin)
- artemisinin
- Anti-fungal drugs such as nystatin
- Hydroxychloroquine, except when used for post-antibiotic Lyme arthritis
- Drugs recommended based on non-human studies, especially those funded by CLD advocates or those peddling treatments for CLD
- Anti-parasitic drugs such as Nitazoxanide (aka Alinia) and Ivermectin
- Anti-babesial drugs (clindamycin, quinine, atovaquone aka Mepron, and experimental anti-babesial drug tafenoquine) without a plausible diagnosis of Babesiosis. Based on sources such as expert recommendations for Lyme and Babesiosis, we conclude:
- Babesia infections should be confirmed via blood smear examination or PCR from a mainstream lab.
- For babesiosis, antibody testing and tests sold by predatory labs should not be used for diagnostic confirmation.
- Standard babesiosis treatment is 7-10 days.
- Longer treatment is typically only recommended in immunocompromised patients.
- “Immunocompromised” includes those without a spleen, people with cancer, those taking immunosuppressive drugs (e.g. rituximab), and those with uncontrolled HIV/AIDS.
- Though symptomatic babesiosis should be treated, people who are younger (e.g. < 50 years old) and not immunocompromised are less likely to have severe illness. These groups can usually clear a Babesia infection without treatment.
- Babesia transmission is even more geographically limited than Lyme disease
- Black legged ticks are the only known vector for Babesia parasites, except for rare transmissions congenitally and via donor blood or transplant.
- As of January 2024, tafenoquine for babesiosis is considered experimental but has been prescribed off-label for severely immunocompromised patients with success and failure.
- Long-term antibiotics
- Spending a substantial sum of money on chronic Lyme treatments and fundraising for them (The cost of real Lyme treatment is typically less than $50 or covered by insurance)
- Non-FDA approved, disproven, or unproven treatments, including: nutritional supplements, herbs, essential oils, colloidal silver, low-dose naltrexone, and homeopathy
- Look for the “Quack miranda warning“
- Examples of supplement/herbal snake oil include Samento/Cat’s Claw, cryptolepis, garlic/allicin, teasel root, monolaurin, Japanese knotweed, berberine, Chinese skullcap, Sida acuta, Houttuynia, oil of oregano, stevia, serrapeptase, NAC (n-acetyl cysteine), and curcumin/tumeric
- strange electrical devices (rife machines, Pulsed Electromagnetic Field-PEMF, BEMER, BioCharger, AmpCoil, Healy, bioresonance, frequency)
- “detoxing” or “cleansing” including taking substances marketed as binders, activated charcoal, Mimosa pudica, detox foot baths
- Hyperbaric oxygen (HBOT), ozone, stem cell therapy, exosomes, bee venom therapy, drinking urine, chelation, coffee enemas or colonics, Supportive Oligonucleotide Therapy (SOT) (aka anti-sense oligonucleotide therapy and Supportive Oligonucleotide Technique), peptide therapy, IVIG (intravenous immunoglobulin), Induced Native Phage Therapy (INPT), ultraviolet light treatments (UVLrx), Lyme laser treatments, plasmapheresis and attempts to “clean” the blood, Insulin Potentiation Therapy (IPT)
- Fever and warming treatments, such as infrared sauna and hyperthermia
- Infamously, some Lyme quackery victims were injected with malaria
- Unnecessary intravenous treatments, including installation of a PICC line
- Including IV vitamins such as glutathione, NAD+, vitamin C, and Myers cocktail
- There have been deaths from IV hydrogen peroxide and intravenous ozone (“autohemotherapy”), both of which have no legitimate medical purpose.
- A belief that “herxing” is occurring when this is implausible, for example not being within 24-48 hours of taking antibiotics for the first time.
- Claims that various quack-diagnosed conditions (often called co-infections) need to be treated one at a time rather than simultaneously. An example from one chronic Lyme cult member: “Now I’m paying out of pocket for an LLMD. She found so many other things that she is having to take into account in my treatment. We’re going to have to repair my immune system before attacking Lyme and repair my hormones and thyroid.”
- “Detoxing,” attempts to “boost the immune system,” unnecessary diets (organic, non-GMO, gluten- free, dairy-free except when taking doxycycline, tomato-free, paleo, keto/ketogenic, sugar-free, carnivore), starvation diets (sometimes marketed as water fasting or dry fasting)
- Treatment protocols named after people (e.g. Stephen Harrod Buhner, QingCai Zhang, Trevor Marshall, Wiegman, William Lee Cowden, Byron White, Bill Rawls, )
- Unnecessary dental work (e.g. removal of fillings)
- Advocacy for more than a single dose of doxycycline after a tick bite where there are no signs of tick-caused illness. Experts only recommend a single dose of doxycycline for high-risk attachments.
{kind=link}
Social and Identity Red Flags
- Adopting the “Lyme warrior” identity
- Multiple family members with dubious diagnoses, including a child who may become a victim of Medical Child Abuse
- Hostility towards science-based medicine, infectious disease experts, and organizations like the CDC
- Relying on low quality evidence such as non-human studies, anecdotes, and studies without control groups
- Referencing doctors and scientists who are financially invested in chronic Lyme disease. They may receive funding from chronic Lyme advocacy groups, be chronic Lyme patients themselves, or make money selling selling tests and treatments.
- Protecting “Lyme literate” doctors (cult leaders aka LLMDs) at all costs, including not mentioning the name of their doctor
- Starting or contributing to a web site, organization, or social media page to raise “awareness” and evangelize for chronic Lyme disease
- Encouraging everyone to watch propaganda videos such as Under Our Skin and The Quiet Epidemic
- Trying to convince sick people that they have Lyme disease and referring them to “Lyme literate” quacks, predatory labs selling non-recommended testing, and snake oil treatments
- Promoting false and misleading information about Lyme disease
- Talking about “biofilms,” “persisters,” intracellular, or “cyst forms,” which are not real problems with Lyme disease
- Receiving medical advice from an individual who also received one or more dubious diagnoses
- Promoting government policies and legislation that support chronic Lyme quackery and hobble consumer protection laws
- Other conspiracy theorist beliefs (e.g. demonizing vaccines, especially the safe and effective Lyme vaccine Lymerix)
- Wishing that those skeptical of chronic Lyme disease be bitten by ticks and get a disease
- Inappropriately comparing Lyme disease to other health issues, such as AIDS, cancer, tuberculosis, syphilis, and acne.
- Using the term “remission” in relation to Lyme disease (which is an easily cured infection in reality)
- Promoting videos or photos of treatment regimens (See photo of reality TV personality Yolanda Hadid for an example.)
- Including saving treatment paraphernalia such as pill bottles or syringes for purposes of drawing attention.
- Developing or joining a for-profit business selling chronic Lyme quackery
- Examples include joining an MLM scheme and partnering with or becoming a “Lyme literate” practitioner
More resources:
Dr. Edzard Ernst: Six signs you are being treated by a quack
Dr. Steven Novella: The Bait and Switch of Unscientific Medicine
Dr. David Weinberg: Anecdotes: Cheaper by the Dozen
Sci-ence.org: Red flags of quackery
The Logic of Science: The hierarchy of evidence: Is the study’s design robust?
Dr. Harriet Hall: How to Talk to People About CAM
Hormones Demystified: Top 10 Reasons Why Smart People Are Stupid About Their Health
Janja Lalich, Ph.D. & Michael D. Langone, Ph.D.: Characteristics Associated With Cults
Review by Allen Steere and colleagues: Lyme borreliosis (See Box 2: Therapies not recommended for Lyme borreliosis or PTLDS)
Review by Paul Lantos and colleagues: Unorthodox alternative therapies marketed to treat Lyme disease
Updated February 4, 2026